
The transition of a resident from a hospital to a nursing home is a significant and often complex event. Effective communication and documentation are crucial for ensuring the resident's safety, comfort, and well-being. A well-structured nursing home progress note template provides a standardized framework for capturing essential information, facilitating collaboration among healthcare professionals, and providing a clear record for continuity of care. This article will delve into the key components of a robust progress note template, exploring its purpose, structure, and best practices for effective use. Nursing Home Progress Note Template – a cornerstone of quality care, it's more than just a document; it's a vital tool for maintaining a resident's dignity and promoting a positive experience.
Understanding the Purpose of a Progress Note
The primary purpose of a nursing home progress note is to comprehensively document a resident's condition, activities, and any changes observed over a specific period. It's a record of what's happening, what's been done, and what needs to be addressed. This information is invaluable for:
- Healthcare Team Collaboration: It allows nurses, doctors, therapists, and social workers to share a consistent understanding of the resident's needs.
- Care Planning: The notes provide a foundation for developing and implementing individualized care plans.
- Patient Safety: Detailed records can identify potential risks and proactively address them.
- Billing and Insurance: Accurate documentation is essential for proper billing and insurance claims.
- Resident's Dignity and Peace of Mind: A clear and informative note demonstrates that the resident's needs are being met and that their care is being actively managed.
The Essential Components of a Progress Note
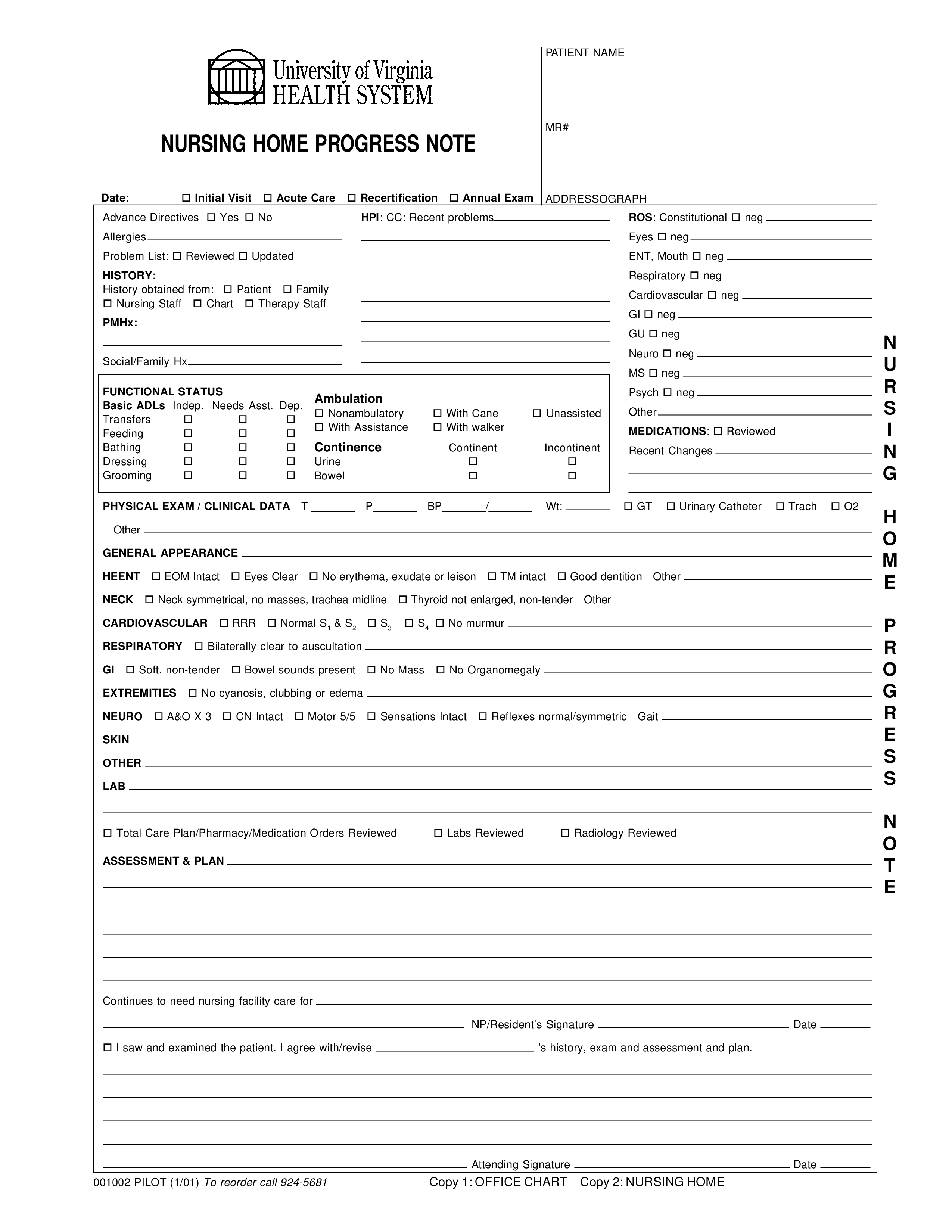
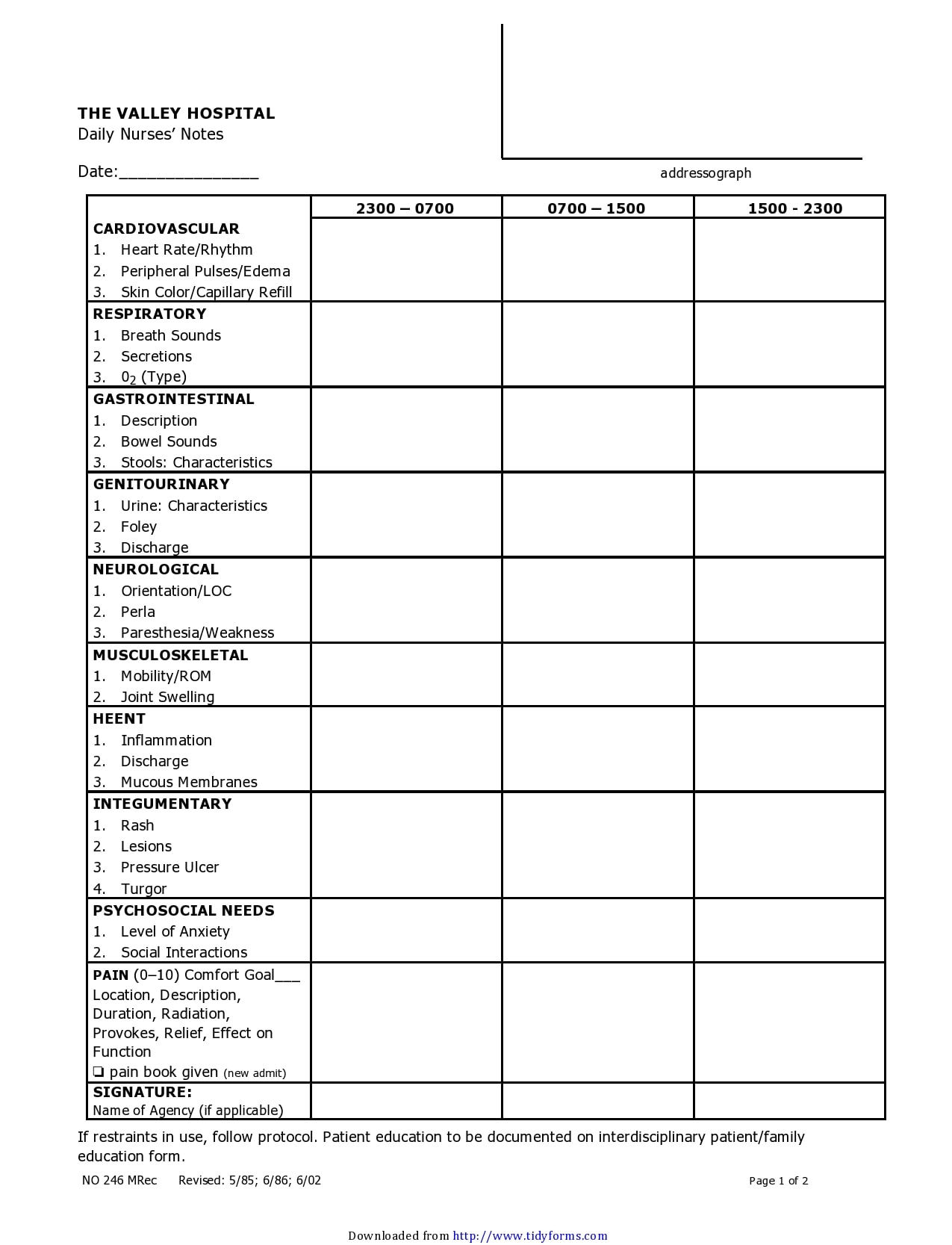
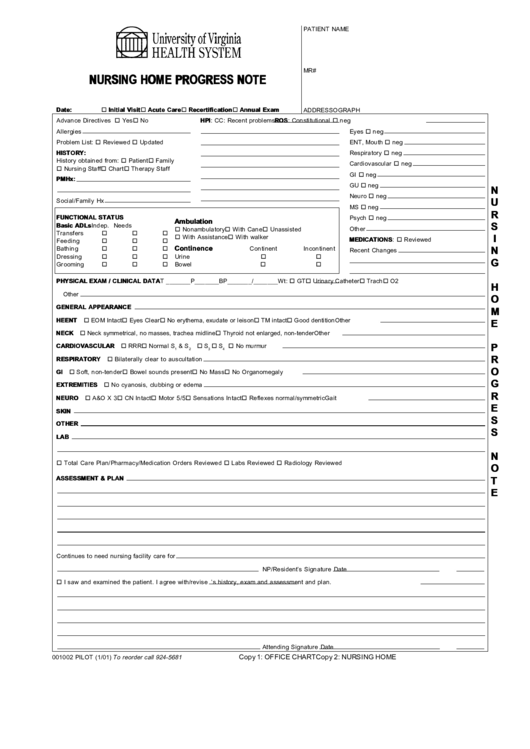
A comprehensive nursing home progress note typically includes the following sections:
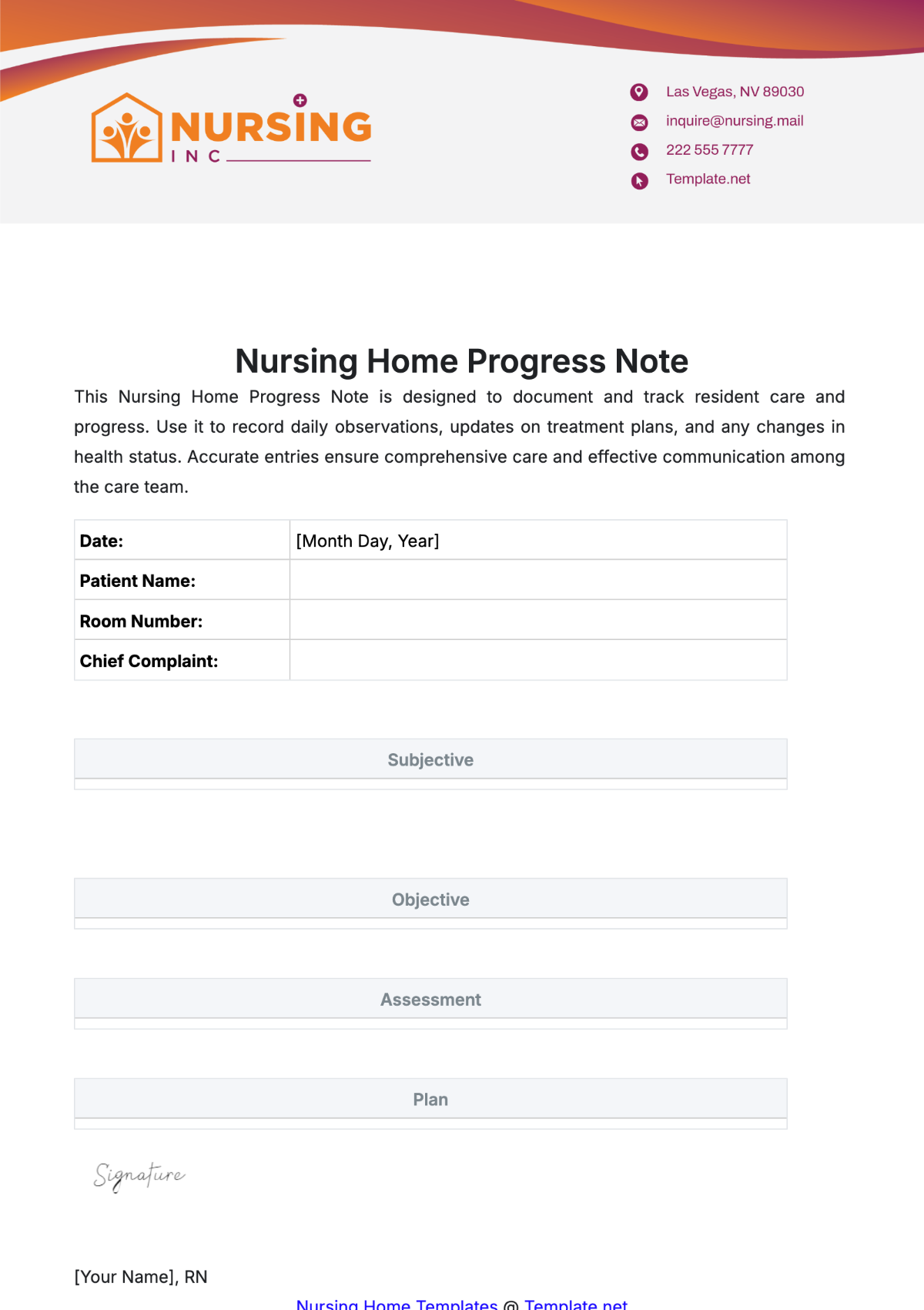
- Patient Demographics: This section includes the resident's full name, date of birth, address, contact information, and any relevant medical history.
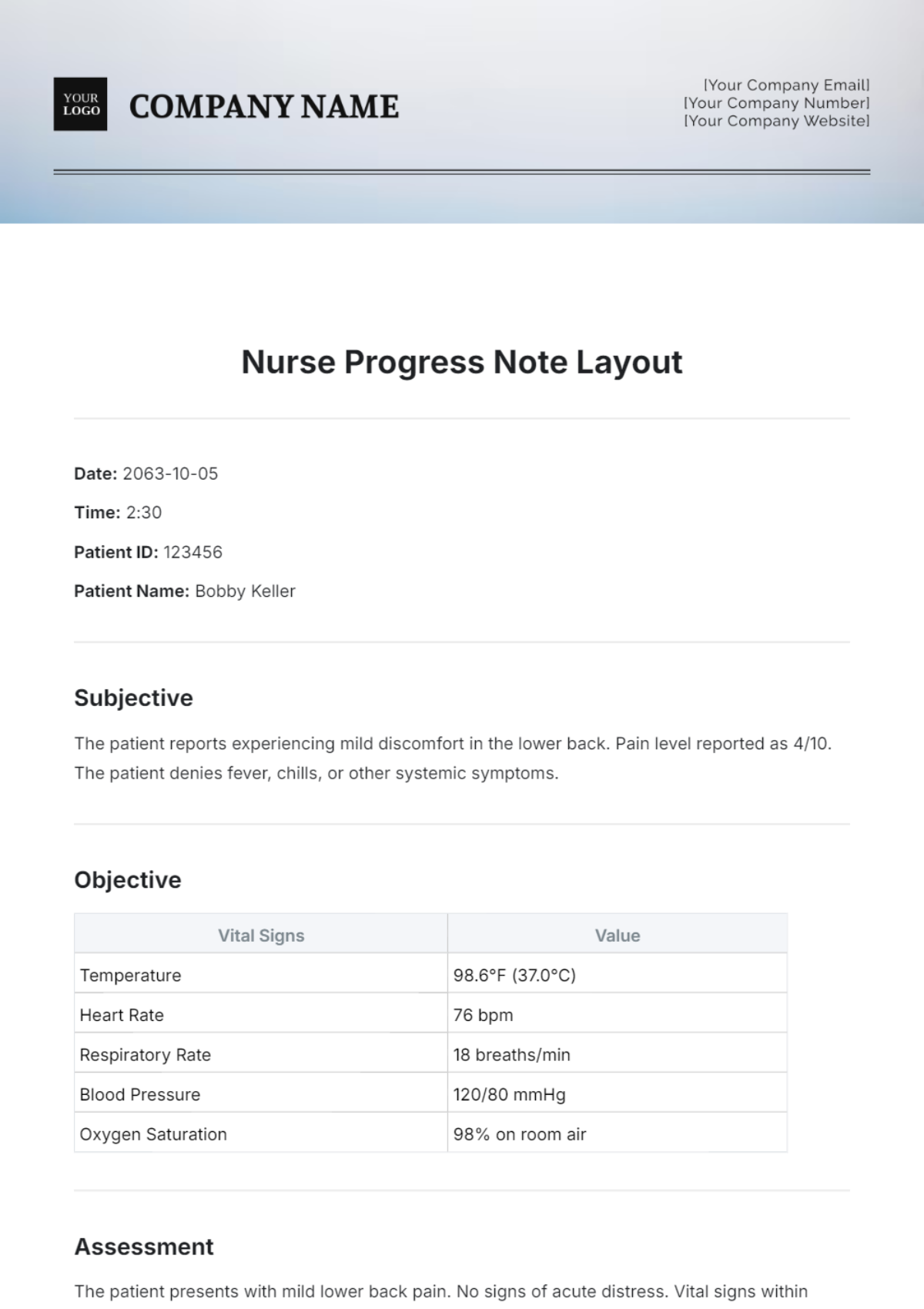
- Date and Time of Visit: Record the precise date and time the note was completed.
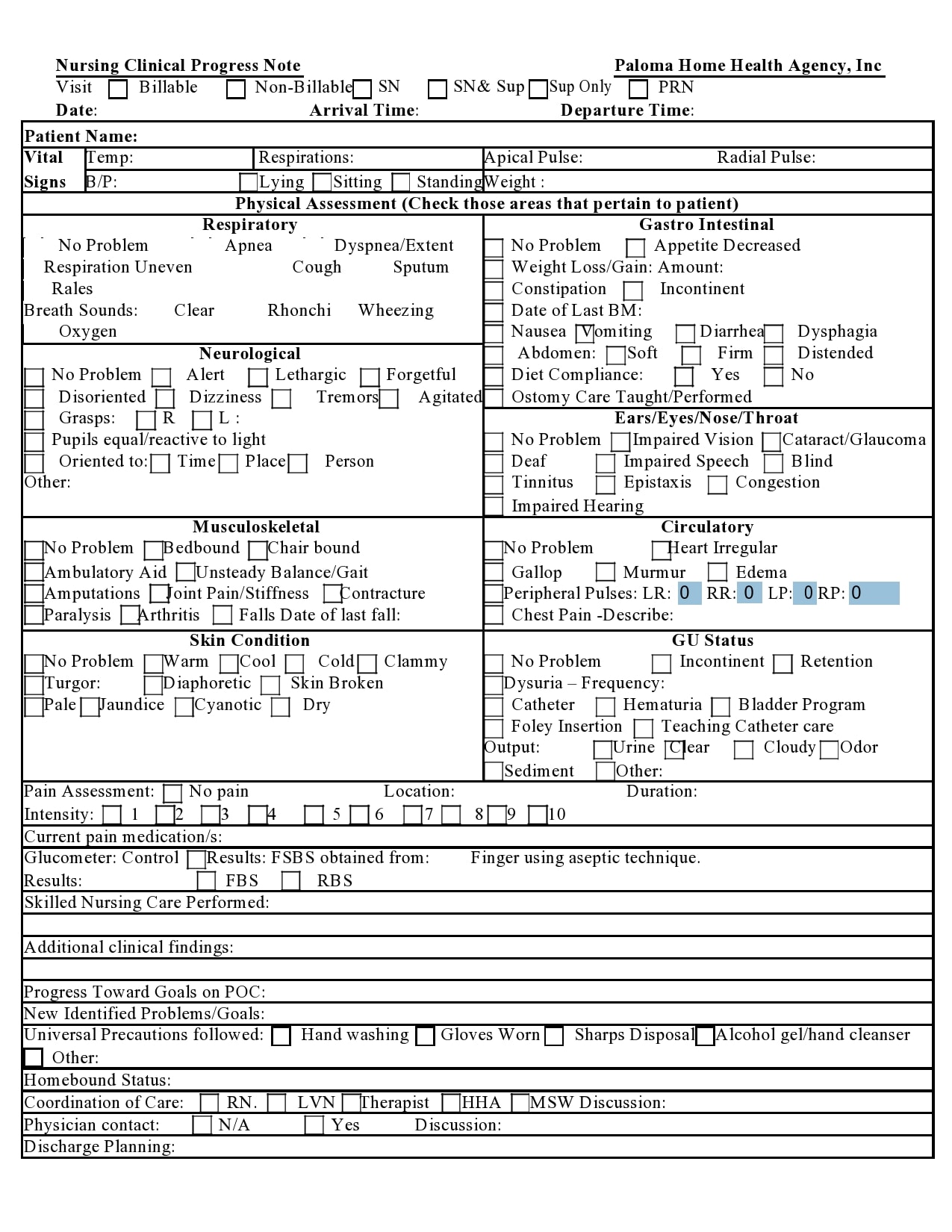
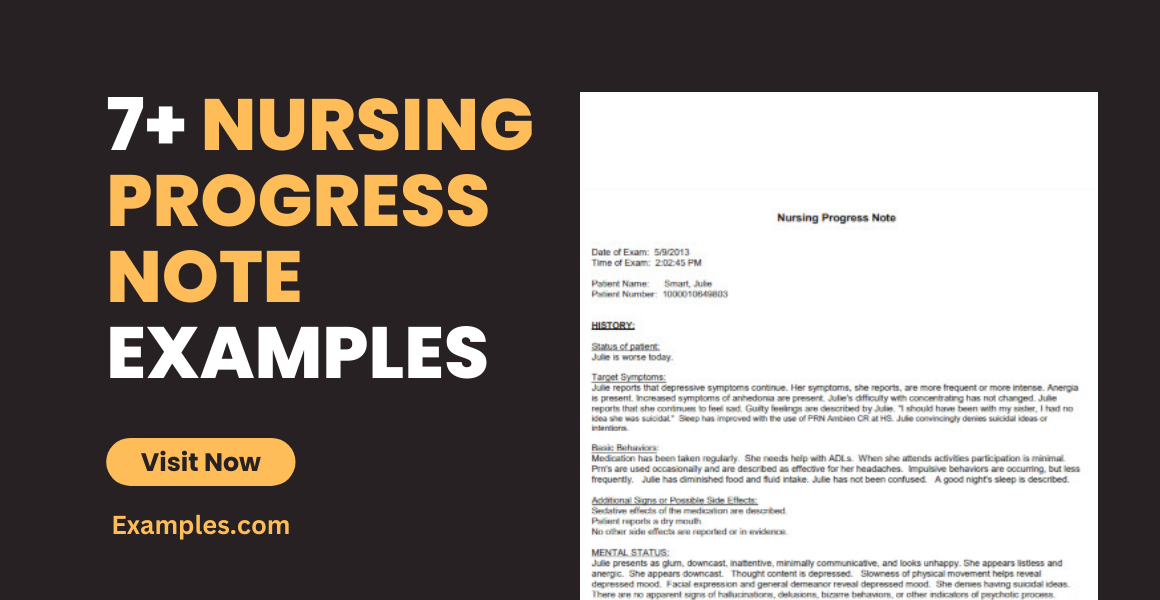
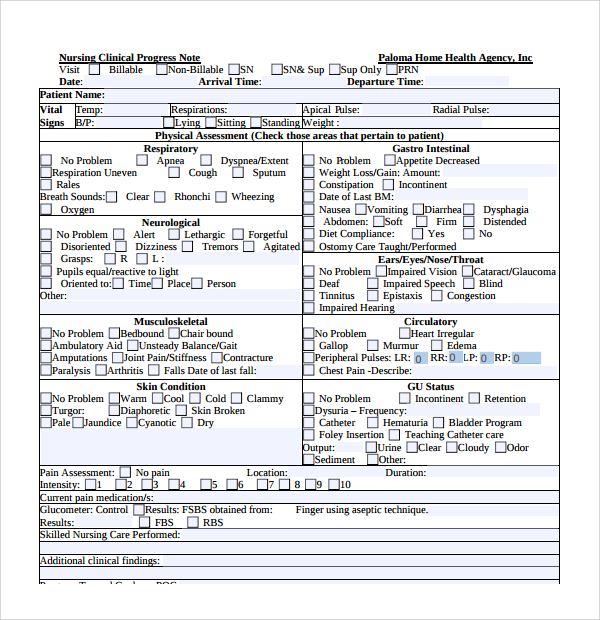
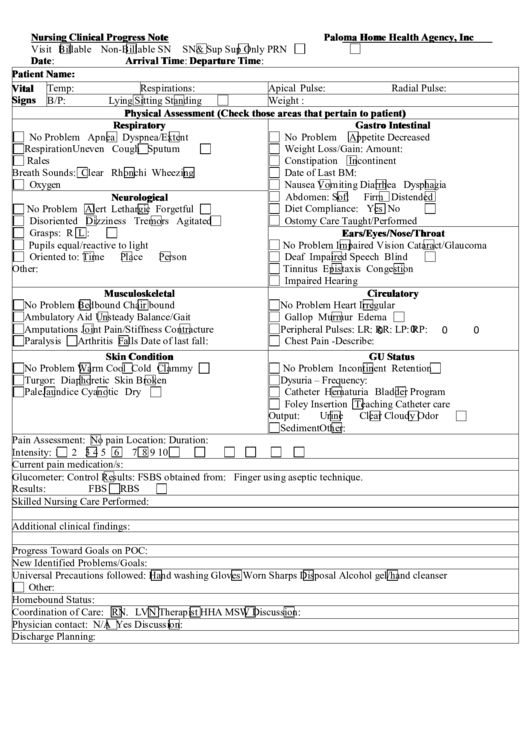
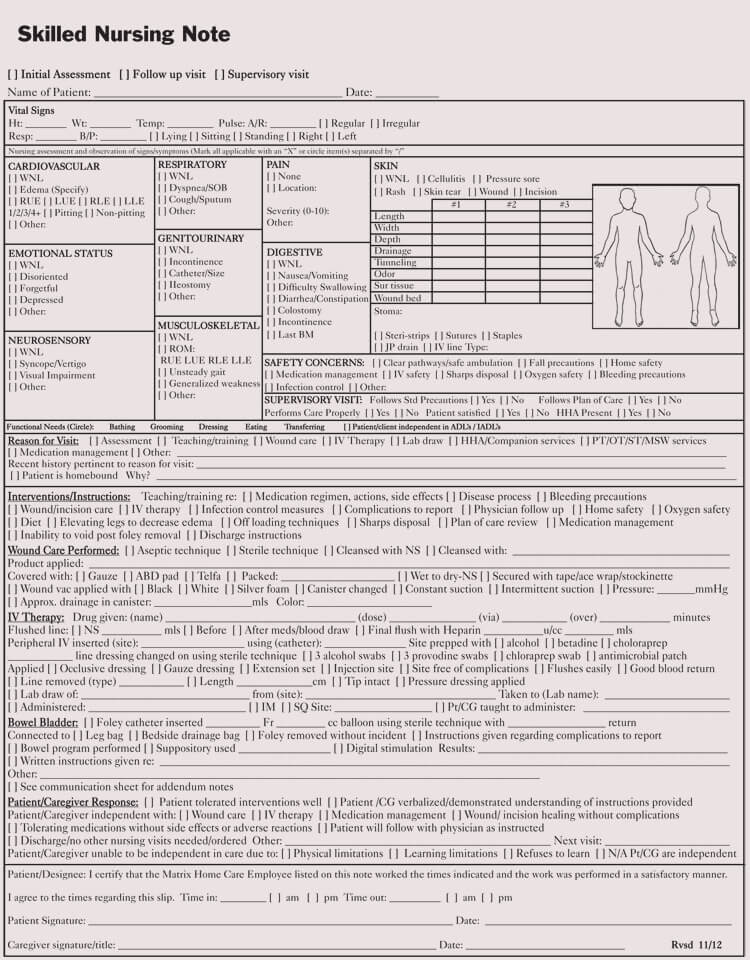
- Observations: This is the core of the note, detailing what the healthcare team observed during the visit. It should be objective and factual, avoiding subjective interpretations.
- Functional Status: A description of the resident's ability to perform activities of daily living (ADLs) such as bathing, dressing, eating, toileting, and mobility.
- Medication Administration: Record all medications administered, including dosage, route, and time. Note any side effects or concerns.
- Dietary Intake: Document the resident's food intake, including the type and amount of food consumed.
- Activities & Engagement: Record any activities the resident participated in, such as exercise, social interaction, or hobbies. Assess their level of engagement and enjoyment.
- Emotional and Psychological Status: Note any changes in mood, behavior, or emotional expression. Be mindful of privacy and confidentiality.
- Changes from Previous Visit: Document any significant changes in the resident's condition, needs, or behavior compared to the previous visit.
- Plan of Care: A brief summary of the care plan in place for the resident, outlining goals and strategies.
- Signature and Date: The note should be signed and dated by a qualified healthcare professional.
Detailed Sections and Examples
Let's examine some of these sections in more detail, with examples illustrating how to incorporate the Nursing Home Progress Note Template into the documentation:
1. Patient Demographics:
"Jane Doe, DOB: 01/15/1948, Address: 123 Main Street, Anytown, USA. Contact: (555) 123-4567. Resident is currently receiving care at Willow Creek Nursing Home."
2. Observations:
"Resident exhibited increased restlessness throughout the morning. She was attempting to move around the room, but was unable to maintain balance. She also appeared to be experiencing mild discomfort in her right hip. The nurse observed her attempting to reposition herself, but she was resistant. A gentle prompt was used to encourage her to move."
3. Functional Status:
"Resident is currently able to ambulate with assistance, but struggles with stairs. She is able to feed herself with minimal assistance. She is experiencing difficulty with dressing, requiring assistance with each step. Her ability to perform activities of daily living is currently limited."
4. Medication Administration:
"Received 10mg of Lisinopril, 50mg every 6 hours, by oral route. Patient reported no adverse effects. Patient was instructed to monitor for signs of hypotension."

5. Dietary Intake:
"Received a light breakfast of oatmeal and fruit. Patient consumed approximately 60% of her allotted daily caloric intake. She expressed a preference for a small serving of yogurt."
6. Activities & Engagement:
"Resident participated in a 30-minute exercise session, focusing on range of motion exercises. She showed some enjoyment, but was somewhat fatigued. She engaged in a conversation with the social worker about her grandchildren."
7. Emotional and Psychological Status:
"Resident appeared somewhat anxious during the afternoon. She expressed concerns about her mobility and the changes in her surroundings. The nurse offered reassurance and encouraged her to focus on the positive aspects of her care."
8. Changes from Previous Visit:
"Resident's ability to perform toileting was significantly improved during the previous visit. She demonstrated increased confidence and independence in this area. However, she still requires assistance with bathing."
9. Plan of Care:
"The plan of care includes continued physical therapy to improve mobility and balance. Social activities will be scheduled to promote engagement and reduce feelings of isolation. A fall prevention assessment will be conducted to identify and address any potential risks."
Conclusion
A well-structured nursing home progress note template is an indispensable tool for providing comprehensive and accurate documentation. By consistently utilizing this template and focusing on objective observations, healthcare professionals can ensure that residents receive the best possible care, promoting their well-being and facilitating a positive transition to a new environment. Regular review and updating of the template are essential to maintain its effectiveness and adapt to the evolving needs of the resident population. Ultimately, the goal is to create a record that empowers caregivers and supports the resident's quality of life.
Conclusion
The transition to a nursing home represents a significant shift for a resident, and effective communication and documentation are paramount to ensuring a smooth and supportive experience. A thoughtfully constructed progress note template, incorporating detailed observations, functional assessments, and a clear plan of care, provides the foundation for collaborative care and promotes resident dignity and peace of mind. By prioritizing accuracy, objectivity, and a focus on the resident's needs, healthcare providers can significantly enhance the quality of care provided within the nursing home setting.
0 Response to "Nursing Home Progress Note Template"
Posting Komentar